On occasion, I hear feedback that the ADL Balance Trainer is not "functional." We clearly promote it as a functional training product, heck it is even part of its' name. So where is the disconnect?
The "not functional" argument usually centers around 2 points: the use of plastic cones and the fact that is not an actual activity of daily living (ADL): cooking, cleaning, washing, etc.
The criticism that the Trainer does not include actual ADLs is TRUE. It was never designed to replace ADL training, rather to facilitate it. In skilled rehab setting, very few patients are able to safely stand and complete real ADLs (if they were, then they would be discharged home). Due to various neurological and/or orthopedic reasons, patients lack the physical ability (strength, balance, stamina, coordination/control, etc.) to stand without hand support, let alone to safely stand and move (reach, bend, twist, etc.), which is key to completing actual ADLs. This is where the ADL Balance Trainer really shines. It is designed for therapists get close and personal with patients in standing. It makes it easy to assist, coach, facilitate, support, and block postures and movements from the front - which is impossible to do at a table or counter top because structures are in the way (see post WARNING: Keep Balance Trainer Away From Walls for more information). This proximity also helps patients feel safe when relearning how to stand and balance (more on this topic in post titled Unable to Stand Without Help? The ADL Balance Trainer Can Help).
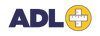
In respect to the argument about cones not being functional. Again I agree that we do not handle cones in real ADLs, rather cups, bowls, utensils, clothes, pans, etc. Although therapists are adapting and using these items with the Trainer (see picture below), the inclusion of cones (and rings) came about during prototyping phase. By including colored cones, rings, and platforms, we stumbled on a great way to add motivational and cognitive challenges to balance training. Through the use of colored items, we developed a variety of balance games to challenge visual-perceptual, memory, executive functioning, and more (see page Balance Games and post 7 Areas the ADL Balance Trainer Helps with Cognitive Rehab) for more information). The games are often praised by therapists for engaging patients in exercises and including cognitive challenges for patients recovering from CVAs and TBIs.
Before the ADL Balance Trainer I would use parallel bars to help patients relearn how to stand again without hand support. However, I found that once standing, I did not have a lot of options for improving reaching. With the Trainer, not only can I can sit in front of patients to teach and train on balance, but I can also add reaching up, down, and around. Coincidentally, I often think of the ADL Balance Trainer as parallel bars for ADLs. Parallel bars are great for learning to walk again. In a similar vein, the ADL Balance Trainer is great for learning to perform ADLs again. Just as patients eventually walk outside of the parallel bars, they also get back to real ADLs without the Trainer.
Hopefully this post adds clarity to why the ADL Balance Trainer is functional. It is unmatched in its' ability to help progress patient toward real ADLs and hopefully back to safe, independent, and fulfilling living.

Photo of ADL Balance Trainer with adaptations by OT to help work with patient on hanging clothes.